A Novel Therapeutic Approach for Managing Hidden Epidemic of FLA1c in Patients with T2DM
Non-alcoholic fatty liver disease (NAFLD) affects up to one-third of the general population worldwide. Type 2 diabetes mellitus (T2DM) and obesity are present in more than half of these patients. (1) A recently conducted Indian study reported that the incidence of NAFLD among individuals with diabetes is 57.6%. (2)
Setting FLA1c Goals in T2DM: Redefining Approach Towards Improving Liver Fat & HbA1c:
Beyond T2DM and obesity, NAFLD has a significantly higher association with various clinical & biochemical markers such as body mass index(BMI), systolic blood pressure(SBP), diastolic blood pressure(DBP), total cholesterol (TC), triglyceride(TG), alkaline phosphatase(ALP), glutamic oxalacetic transaminase, fasting C-peptide, 2-h postprandial blood glucose (PPBG) homeostasis model assessment (HOMA) of insulin resistance, homeostasis model assessment (HOMA) of insulin secretion as compared to non-NAFLD patients (P<0.05). (3)
Higher glycated hemoglobin (HbA1c) levels have strongly correlated with NAFLD. Asian studies have indicated higher than normal HbA1C, and waist circumference measurements possess a more than 70% potential to predict NAFLD, inferring a close interaction between NAFLD and uncontrolled blood glucose levels (4) Guidelines recommend stringent glycemic control of HbA1c <7%, to reduce the risk of long-term complications in these patients. (5)
There is a strong need to consider an aggressive multipronged treatment approach for the management of T2DM with NAFLD. These include targeting HbA1c, hepatic fat content, insulin resistance, liver enzymes, and lipid parameters for optimizing treatment care outcomes. Hence, the treatment may need to be aimed at understanding the importance of managing the core parameters associated with fatty liver (FL) and HbA1c, a clinical concept amalgamating as targeting “FLA1c” in T2DM patients with NAFLD.
Several studies have insightfully stressed that certain currently available therapies targeting insulin resistance and hepatic fat, such as Pioglitazone and Vildagliptin, might be relevant considerations to improve both hepatic and metabolic outcomes. (6)
Achieving FLA1C Goals: Rationale for Considering Vildagliptin-Pioglitazone Combination in Diabetes Patients with NAFLD
Pioglitazone, an insulin-sensitizer, targets insulin resistance and adipose tissue dysfunction or inflammation that promotes hepatic "lipotoxicity" in non-alcoholic steatohepatitis (NASH) and is also a prominent feature of T2DM, makes it clinically helpful in treating steatohepatitis in this population. (7)
Pioglitazone treatment also improved parameters of liver histology, like ballooning degeneration, lobular inflammation, steatosis, and combined necroinflammation in patients with NASH. (8)
Acknowledging the potential of Pioglitazone, the American Association of Clinical Endocrinology 2022 clinical practice guideline in association with the American Association for the Study of Liver Diseases (AASLD) recommend using Pioglitazone in individuals with NASH and T2DM (A1) (9). Indian National Association for Study of the Liver (INASL) also recommended pioglitazone as pharmacotherapy for NASH with or without hepatic fibrosis (F1–F3) in both diabetic and nondiabetic adult patients (I, Strong). (10)
Dipeptidyl-peptidase-4 (DPP-4) plays a crucial association in various chronic liver diseases, as high plasma DPP-4 activity is reported in T2DM with NAFLD. Vildagliptin- an incretin-based oral antidiabetic agent used in patients with T2DM- is known to decrease insulin resistance and plasma DPP-4 activity, both of which positively correlated with improvement in liver enzymes. (11)
In addition to Vildagliptin’s glucose-lowering efficacy, treatment with vildagliptin can reduce lipid parameters like TC, TG, and low-density lipoprotein cholesterol (LDL-C) in T2DM with NAFLD. (11)
Vildagliptin treatment led to a reduction in aminotransferase levels, alanine aminotransferases, and aspartate aminotransferases levels. It is noteworthy that about 65.5% improvement in fatty liver grading on ultrasound assessment was observed with vildagliptin treatment among NAFLD patients. These pieces of evidence are more meaningful for Indian clinicians as they were replicated in Asian studies. (11)
The RSSDI (2022) guideline also recommends DPP4 inhibitors such as Vildagliptin, including in diabetes management. The weight neutrality and higher efficacy in Asians, in general, and Indians, in particular, define the role of the drug in T2DM. (12)
Clinical Evidence for Using Pioglitazone & Vildagliptin in Diabetes Patients with NAFLD
Clinical Benefits of Pioglitazone:
Pioglitazone inhibits hepatic fatty acid synthesis, remodelling adipose tissue to sequester fatty acids and promoting insulin sensitivity by increasing adiponectin levels and decreasing proinflammatory cytokines. (1)
The findings from a meta-analysis including 26 studies (n=946 NAFLD patients) demonstrated significant improvements with Pioglitazone, particularly in transaminases and liver histology in diabetic and non-diabetic NAFLD patients. Pioglitazone reduced alanine aminotransferases (MD -38.41, p<0.001) and significantly improved liver steatosis (SMD -1.01; p<0.001). This suggests the efficacy of Pioglitazone in improving transaminases and liver histology in diabetic and NAFLD patients. (1)
Another double-blind randomized study (n=251) also showed that treatment with Pioglitazone has been clinically proven to reduce HbA1c by 1.05%, and fasting blood glucose (FBG) by 36 mg/dl. (13)
A study published in the New England Journal of Medicine reported that treatment with pioglitazone and dietary changes, as compared with only dietary modifications plus placebo, among patients with NASH improved glycemic control and glucose tolerance (P<0.001), normalized liver aminotransferase levels as it decreased plasma aspartate aminotransferase levels (40% vs 21%, P = 0.04), decreased alanine aminotransferase levels (58% vs 34%, P<0.001), decreased hepatic fat content (54% vs 0%, P<0.001), and increased hepatic insulin sensitivity (48% vs 14%, P = 0.008). Patients showed significant improvement in histologic improvements in all variables, including inflammation ballooning necrosis, steatosis, and fibrosis. The combined necroinflammation score improved in 85% of patients with pioglitazone, as compared with 38% of those who received a placebo. (14)
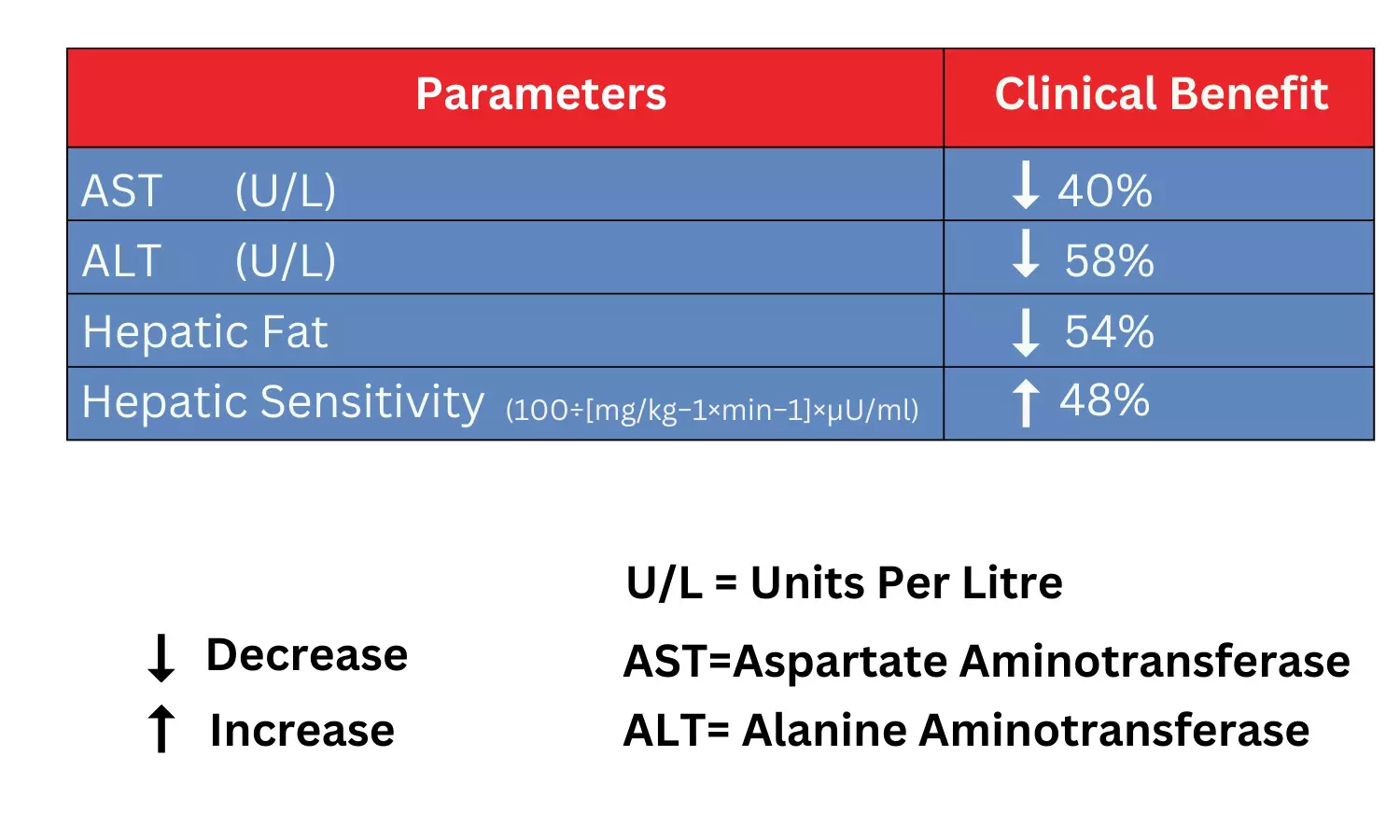
Changes in liver parameters in NAFLD. Adapted from Belfort R et al. A placebo-controlled trial of pioglitazone in subjects with nonalcoholic steatohepatitis. N Engl J Med. 2006;355(22):2297-2307.
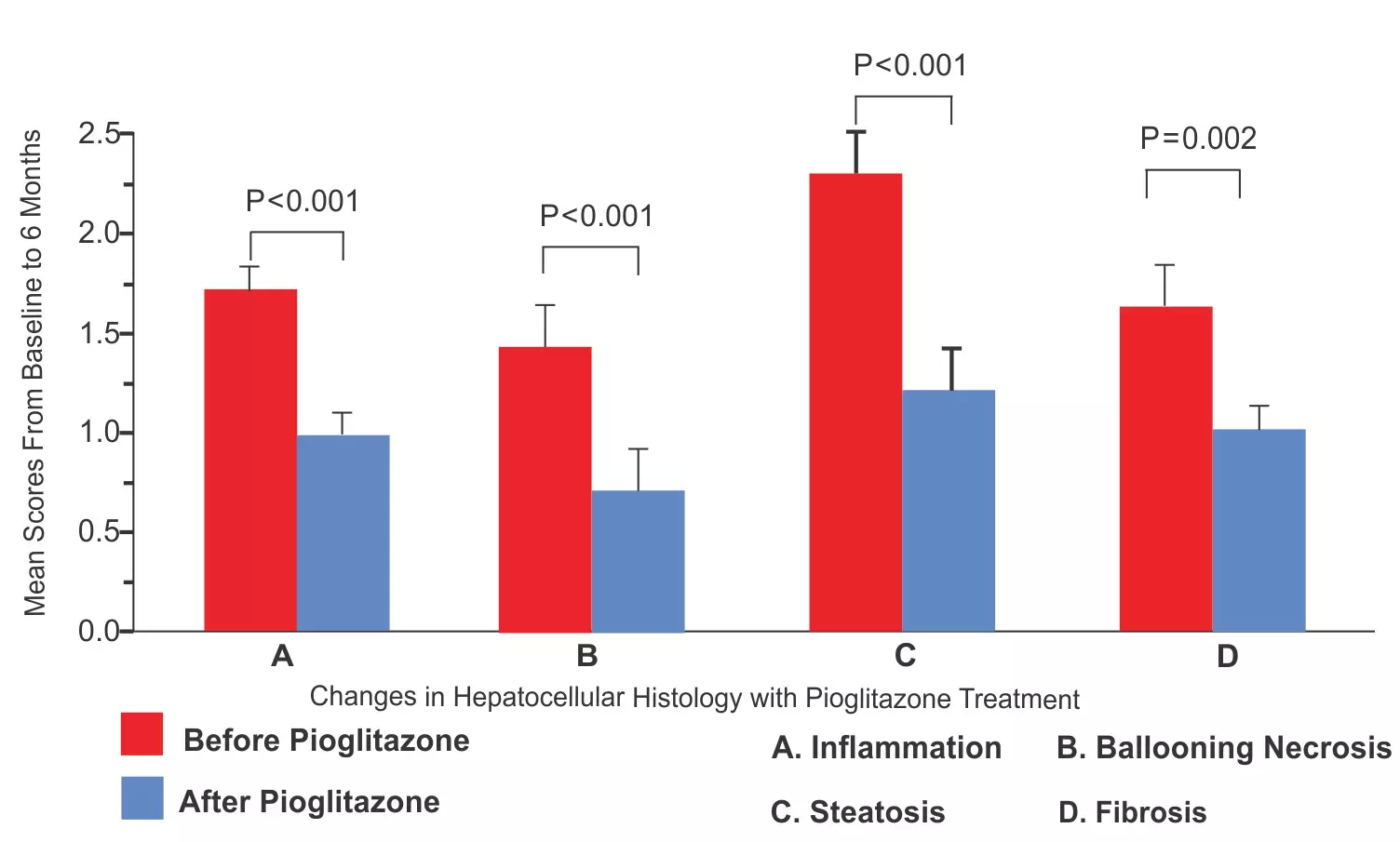
Mean Scores for Inflammation, Ballooning Necrosis, Steatosis, and Fibrosis in Liver Biopsy Specimens with Pioglitazone. Adapted from Belfort R et al. A placebo-controlled trial of pioglitazone in subjects with nonalcoholic steatohepatitis. N Engl J Med. 2006;355(22):2297-2307.
Clinical Benefits of Vildagliptin:
Vildagliptin has beneficial effects on all those risk factors associated with NAFLD, such as improvement in metabolic syndrome, blood pressure, weight gain, and lipid profiles. It also plays an essential role in preventing the progression and complications of NAFLD with its anti-inflammatory and antioxidant properties. Vildagliptin is an oral antidiabetic incretin-based therapy used in patients of T2DM with a well-tolerated profile and no risk of weight gain and hypoglycemia. (11) Long-term treatment with Vildagliptin 50 mg once daily led to an HbA1c reduction of 0.5% without any reported incidence of hypoglycemia over a period of 2 years. (15)
Benefits of Initial Pioglitazone and Vildagliptin Combination:
A 24-week, multicentre, randomized, double-blind, active-controlled study conducted across 154 centres across eight countries, including India, assessed the effects of vildagliptin, pioglitazone, and a combination of the two among 607 drug-naive patients with T2DM. The results demonstrated HbA1c reduction of up to 1.9% and FBG reduction of 50.4 mg/dl in the vildagliptin combined with pioglitazone treatment arm, significantly higher than individual monotherapy treatments. The study concluded that first-line treatment with pioglitazone/vildagliptin combination in patients with T2DM provides better glycaemic control yet has minimal risk of hypoglycaemia and a tolerability profile comparable with component monotherapy. (16)
A post hoc analysis on Korean patients with T2DM of the same study, published later, reported an HbA1c reduction of up to 2.03%, with about 76% of patients achieving the recommended target HbA1c < 7% with combination treatment pioglitazone and vildagliptin over 24 weeks treatment period. (17)
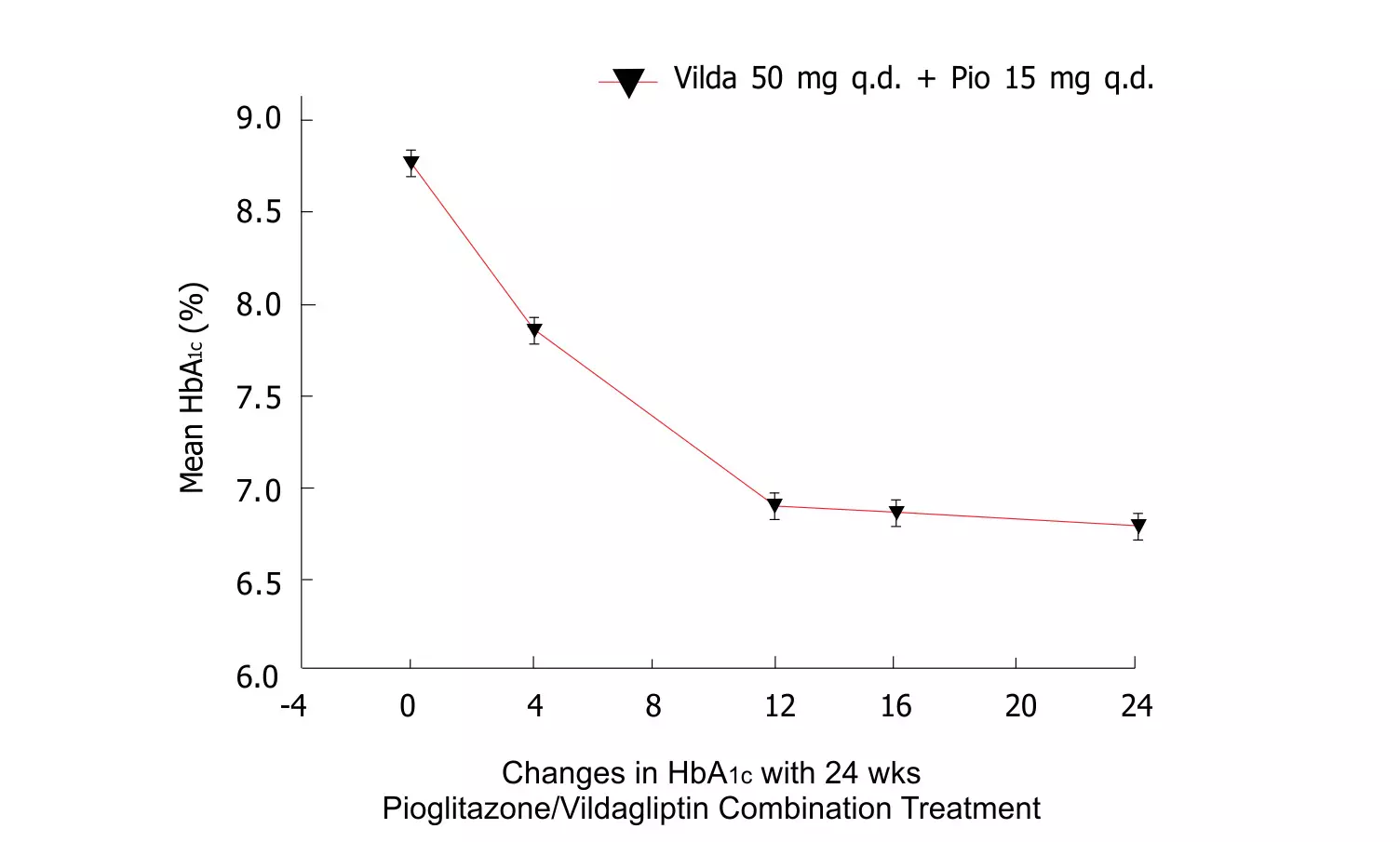
Mean HbA1c during 24-wk treatment with vildagliptin/pioglitazone combination. Adapted from Kim SW et.al. Efficacy and safety of vildagliptin/pioglitazone combination therapy in Korean patients with diabetes. World J Diabetes. 2010;1(5):153-160.
Take Home Message:
✔ Every 1 out of 2 Indian patients with diabetes may be at risk or suffering from NAFLD.
✔ There is a well-defined concurrent and bidirectional relationship between the development of T2DM and the development and progression of NAFLD.
✔ For such a massive group of T2DM population with comorbid NAFLD, there is a need to specifically define a multipronged approach targeting the interconnected pathophysiology at multiple levels in these patients
✔ It may be prudent to consider tackling HbA1c, lipid parameters, and liver enzymes along with improving NAFLD disease activity and liver fat content, which forms the core culprit of a myriad of metabolic dysfunctions in this patient population. Thus, the treatment goals can be set towards achieving 'FLA1c' goals to improve treatment care outcomes.
✔ Clinical studies have shown that Pioglitazone and Vildagliptin effectively treat NAFLD diabetic patients with glycaemic and beyond glycaemic benefits. While pioglitazone aids in long-term metabolic and histologic improvement, Vildagliptin treatment has reported decreased hepatic fat content and serum transaminase levels in NAFLD patients. Pioglitazone and vildagliptin combination studies, including a subset of Indian patients, have been cited in scientific literature.
✔ Guidelines recommend considering the use of Pioglitazone in individuals with NASH and T2DM
✔ The combination of Pioglitazone and Vildagliptin that aims at achieving FLA1c goals may be a novel consideration for the management of NAFLD with T2DM.
References:
1. Kumar J, Memon RS, Shahid I, et al. Antidiabetic drugs and non-alcoholic fatty liver disease: A systematic review, meta-analysis and evidence map. Dig Liver Dis. 2021;53(1):44-51.
2. Kumar P, Rawat S, Kakar A, Sinha AK. Prevalence of non-alcoholic fatty liver disease among diabetes, prediabetes, and healthy population. J Family Med Prim Care. 2022;11(12):7640-7643.
3. Ren, W., Feng, Y., Feng, Y. et al. Relationship of liver fat content with systemic metabolism and chronic complications in patients with type 2 diabetes mellitus. Lipids Health Dis 22, 11 (2023).
4. Masroor M, Haque Z. HbA1C as a Biomarker of Non-alcoholic Fatty Liver Disease: Comparison with Anthropometric Parameters. J Clin Transl Hepatol. 2021;9(1):15-21.
5. Diabetes Care 2021;44(Supplement_1):S73–S84.
6. Xia MF, Bian H, Gao X. NAFLD, and Diabetes: Two Sides of the Same Coin? Rationale for Gene-Based Personalized NAFLD Treatment. Front Pharmacol.2019;10:877. 2019.
7. Cusi K, Orsak B, Bril F, et al. Long-Term Pioglitazone Treatment for Patients With Nonalcoholic Steatohepatitis and Prediabetes or Type 2 Diabetes Mellitus: Randomized Trial. Ann Intern Med. 2016;165(5):305-315
8. Boettcher E, Csako G, Pucino F, Wesley R, Loomba R. Meta-analysis: pioglitazone improves liver histology and fibrosis in patients with non-alcoholic steatohepatitis. Aliment Pharmacol Ther. 2012;35(1):66-75.
9. Cusi K, Isaacs S, Barb D, et al. American Association of Clinical Endocrinology Clinical Practice Guideline for the Diagnosis and Management of Nonalcoholic Fatty Liver Disease in Primary Care and Endocrinology Clinical Settings: Co-Sponsored by the American Association for the Study of Liver Diseases (AASLD). Endocr Pract. 2022;28(5):528-562.
10. Duseja A, Singh SP, De A et Al, Indian National Association for Study of the Liver (INASL) Guidance Paper on Nomenclature, Diagnosis and Treatment of Nonalcoholic Fatty Liver Disease (NAFLD). J Clin Exp Hepatol. 2023 Mar-Apr;13(2):273-302.
11. Hussain M, Babar MZM, Hussain MS, Akhtar L. Vildagliptin ameliorates biochemical, metabolic, and fatty changes associated with non-alcoholic fatty liver disease. Pak J Med Sci. 2016;32(6):1396-1401.
12. Kumar V, Agarwal S, Saboo B, Makkar B. RSSDI Guidelines for the management of hypertension in patients with diabetes mellitus [published online ahead of print, 2022 Dec 15]. Int J Diabetes Dev Ctries. 2022;42(Suppl 1):1-30.
13. Scherbaum WA, Göke B; German Pioglitazone Study Group. Metabolic efficacy and safety of once-daily pioglitazone monotherapy in patients with type 2 diabetes: a double-blind, placebo-controlled study. Horm Metab Res. 2002;34(10):589-595
14. Belfort R, Harrison SA, Brown K, et al. A placebo-controlled trial of pioglitazone in subjects with nonalcoholic steatohepatitis. N Engl J Med. 2006;355(22):2297-2307.
15. W. A. Scherbaum; A. Schweizer; A. Mari; P. M. Nilsson; G. Lalanne; Y. Wang; B. E. Dunning; J. E. Foley (2008). Evidence that vildagliptin attenuates deterioration of glycaemic control during 2-year treatment of patients with type 2 diabetes and mild hyperglycemia.,10(11), 1114–1124
16. Rosenstock J, Kim SW, Baron MA, et al. Efficacy and tolerability of initial combination therapy with vildagliptin and pioglitazone compared with component monotherapy in patients with type 2 diabetes. Diabetes Obes Metab. 2007;9(2):175-185.
17. Kim SW, Baik SH, Yoon KH, Lee HW, Filozof C. Efficacy and safety of vildagliptin/pioglitazone combination therapy in Korean patients with diabetes. World J Diabetes. 2010;1(5):153-160.
from Medical News, Health News Latest, Medical News Today - Medical Dialogues | https://ift.tt/MmhA5zL



Comments
Post a Comment